Interactive HCFA-1500 Form – Box Guide with 837P Mapping
The HCFA-1500 (also known as the CMS-1500) is the standardized claim form used by healthcare providers to submit professional services for reimbursement. This form captures patient, provider, insurance, and claim details and is required by most payers for accurate processing.
Use our Interactive HCFA-1500 Form Tool to explore every section of the claim form. Simply click on any box (0–33) to see what information belongs there and how it maps to the X12 837P 5010 electronic claim format. Each box links directly to our detailed guides with examples, mapping notes, and compliance tips.
Tip: The form is fully keyboard-navigable and mobile-friendly. You can use the Tab key to jump between boxes or hover with your mouse to highlight specific fields. This makes it an excellent training and reference tool for providers, coders, and billers.
Eclaims – Interactive HCFA-1500 Form v1.0.0
Clickable, keyboard-accessible HCFA-1500 form with box-by-box overlays and direct links. Explore each field’s purpose and see precise X12 837P 5010 mappings with real code examples.
Questions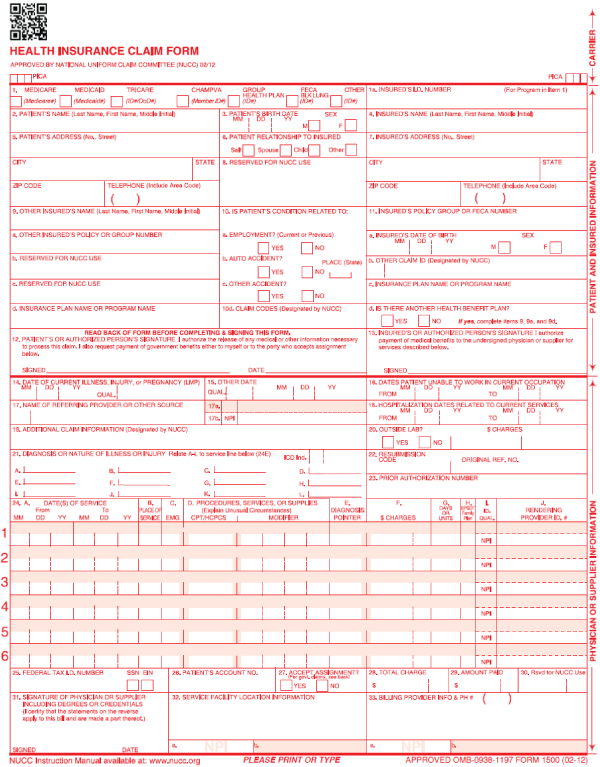
We hope you found this tool useful! Please reach out to us with questions/feedback.
Disclaimer:
While every effort is made to keep all information up to date and accurate, all content found on Eclaims.com is intended to be a general information resource and is provided "AS IS". The accuracy of the information is in no way guaranteed. Eclaims.com makes no warranty to the accuracy, completeness or reliability of any content available through the website. Eclaims.com assumes no liability whatsoever for any errors or omissions in any content contained on this website. You are responsible for verifying any information before relying on it.